
- [email protected]
- +44 (0) 23 8048 3000
FIT Negative Follow-Up
- Resource: Reports
- Date: June 12, 2018
Safety-netting patients with a low faecal haemoglobin concentration and modifying the current patient pathway to improve patient care.
Dr. James Turvill, Consultant Gastroenterologist, York Teaching Hospital NHS Foundation Trust
Dr. James Turvill is a screening endoscopist within the Bowel Cancer Screening Programme and has an interest in inflammatory bowel disease and gastrointestinal cancer. Since 2008 he has developed a research interest in the use of biomarkers to facilitate the diagnosis and monitoring of gastrointestinal disease.
Currently he is working with Y&H AHSN in the implementation of a faecal calprotectin (fCAL) care pathway to support NICE DG11 and with the Y&H Cancer Alliance in the introduction of faecal immunochemical testing (FIT) in patients with suspected colorectal cancer.
In this article Dr. Turvill discusses his study at York Hospital and the importance of negative FIT follow-up for patients.
Read the Full Article Here“NICE guidance is about finding people with cancer so that we can make a difference. FIT should be seen as a technology designed to facilitate this process. So I am a little unsettled about the concept of using FIT as a test to ‘rule-out’ colorectal cancer (CRC), though this is what it is good at. Instead we need to use it to ‘rule-in’ patients and so find CRC early. And here lies the challenge.
In thinking about FIT negative follow up we need to understand what is currently happening in primary and secondary care and then, what a FIT positive result will mean for the future. Then for the FIT negative patient we need to consider consequentialism over essentialism.
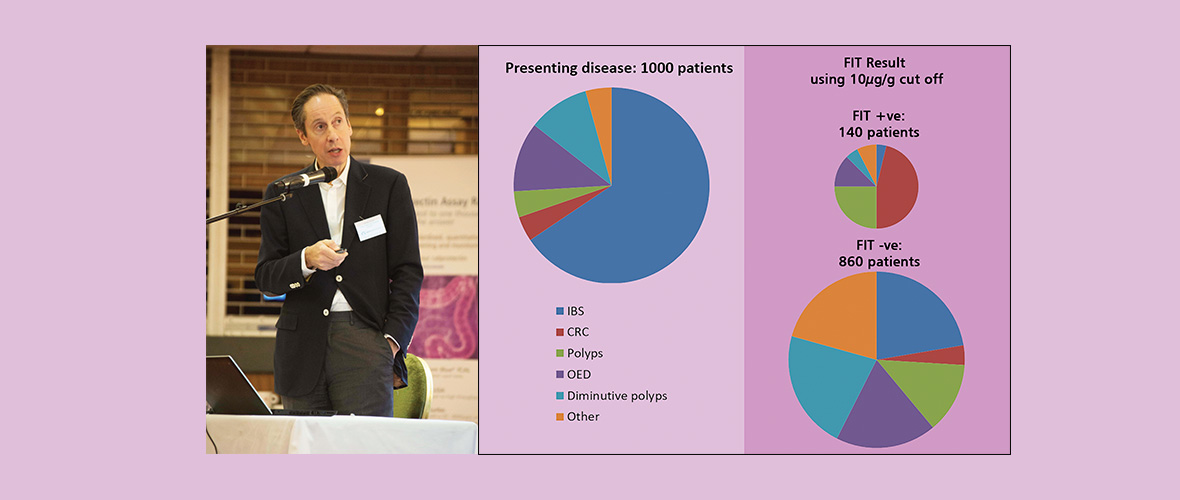
If you look at a cohort of patients referred from primary care fulfilling NICE NG12, that is at high risk of CRC, around two-thirds of patients will have ‘functional disorders’ (predominantly the irritable bowel syndrome (IBS), but also benign anal canal bleeding and iron deficient anaemia of unknown cause). Currently it is this group of patients that secondary care clinicians are focussing on since these are judged to increase healthcare costs by the time constrained consumption of resource in achieving a diagnosis.”
Recent Case Studies

